

{kind=link}
At her baby shower in the summer of 2019, Ava Jones’ smile radiated above the gingham dress that fell snug around her growing belly.
Jones’ pregnancy had been smooth — not even morning sickness — until four days before her due date. That afternoon, she realized that she couldn’t feel her baby move. Jones and her husband, Gregory, rushed to their hospital in Dallas, where she labored for two days before she delivered her stillborn baby.
They named their 6-pound, 4-ounce boy Giles, a nod to his father, who was also named for a saint. When a nurse placed Giles in her arms, he looked like he was sleeping.
“Wake up,” his mother begged. “Please.”
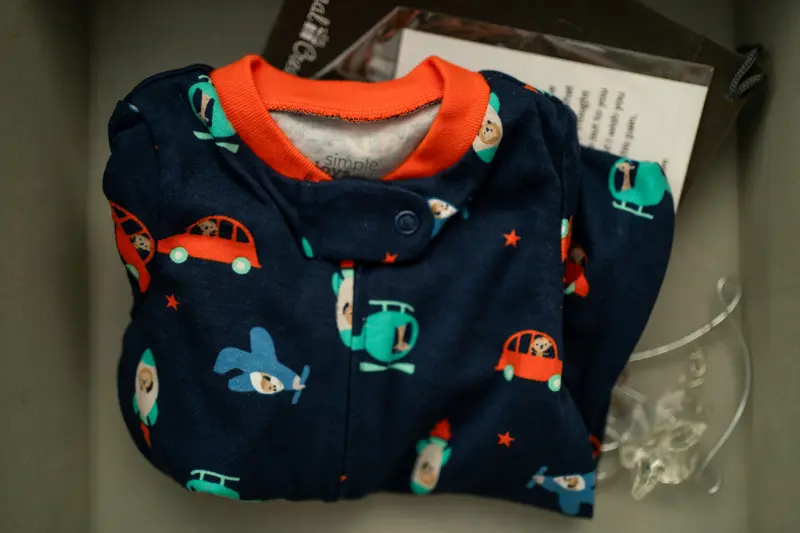
Nearly five years later, the keepsake box for her son has the pajamas they had packed in the hospital bag, a mold of his tiny hand and a small crochet pillow. But what was missing was an official record of his birth. Jones has no fetal death certificate, though Texas requires that one be completed within five days of a stillbirth. She said she was not asked for the necessary information while she was in the hospital and no one there told her how to request the document.

Credit:
Nitashia Johnson, special to ProPublica
From a public health perspective, fetal death certificates provide essential data that helps shed light on stillbirth, the death of an expected child at 20 weeks or more of pregnancy. They serve as the underpinning for much of the research on stillbirth, as well as an evaluation of care in pregnancy and delivery. Tracking the cause of death is key to understanding how to prevent stillbirth, which research shows may be possible in nearly 1 in 4 stillbirths.
ProPublica, which has spent the past two years reporting on stillbirths, has found that state and federal health agencies, lawmakers and local hospitals have failed to prioritize data collection needed to accurately track and understand stillbirth or provide parents with that critical information. Data is frequently incomplete and delayed and is sometimes inaccurate, particularly when it comes to cause of death. Data on stillbirth risk factors and race also is deficient.
And it’s getting worse. A ProPublica analysis of data from the Centers for Disease Control and Prevention for 2019 through 2021 found that the records for more than a third of all 63,437 stillbirths in the U.S. were missing perhaps the most crucial information about the stillbirth: the cause of death. For those stillbirths that happened at 37 weeks or more, that proportion was even higher — and it’s rising, from 41% in 2019 to nearly 44% in 2021.
Even the threshold for reporting a stillbirth is not uniform. Some states use fetal weight as a requirement; others use weeks of pregnancy; some combine the two.
“If we don’t have accurate data, we don’t know the scope of the problem and how to move forward,” said Lauren Christiansen-Lindquist, a maternal and child health epidemiologist and an associate professor at Emory University. “It’s really the foundation of our ability to make any difference in stillbirth rates in the U.S.”
The National Institutes of Health, which last year released a study mirroring ProPublica’s reporting on stillbirth, has started the discussion about improving stillbirth data. In January, the Stillbirth Working Group of Council of the Eunice Kennedy Shriver National Institute of Child Health and Human Development discussed ways to address the data problems, beginning with standardizing the definition of stillbirth across states.
Dr. George Saade, the co-lead of the Stillbirth Working Group’s data subgroup, said the health care system should be set up to give patients accurate information.
“Except we suspend that expectation when it comes to stillbirth. That’s wrong, particularly given that this is such a devastating outcome,” said Saade, who is also chair of obstetrics and gynecology and associate dean for women’s health at Eastern Virginia Medical School. “We’re basically telling them it doesn’t matter.”
State laws require all stillbirths to be reported, and federal law directs the CDC to collect and publish data on stillbirths. That data collection typically begins at the hospital when an employee gathers information from the pregnant person and her medical records; funeral directors and medical examiners may also provide information. That data is sent to the state health department, which ultimately forwards it to the CDC.
But the process is fraught at nearly every level, from untrained hospital staff to state health departments not reporting large amounts of data. The CDC cautioned in a report last year that variation among states’ reporting requirements when it comes to stillbirths “can have implications for data quality and completeness.”
In response to questions from ProPublica, a CDC spokesperson acknowledged challenges with data collection around stillbirths, saying the issue boils down to “lack of resources, which makes it difficult to prioritize fetal death data at both the state and federal levels.”
Improving data collection is a key component to federal legislation championed by maternal health advocate Debbie Haine Vijayvergiya, whose daughter Autumn Joy was stillborn in 2011. The Stillbirth Health Improvement and Education (SHINE) for Autumn Act aims to improve the collection, reporting and timeliness of stillbirth data. It also increases education and awareness and paves the way for research and training in fetal autopsies.
The bill, which would be the most comprehensive stillbirth legislation on record, is still pending in Congress.
“Since Autumn died, I’ve been on this quest to understand why stillbirth has remained a tragically neglected public health crisis and what needs to change to address it,” she said. “I quickly learned how vital good data is in our efforts to improve stillbirth outcomes.”
Minnesota is among the states that have made stillbirth data a priority. A small team there is responsible for data quality, which includes following up with hospitals if the fetal death information it receives is missing information.
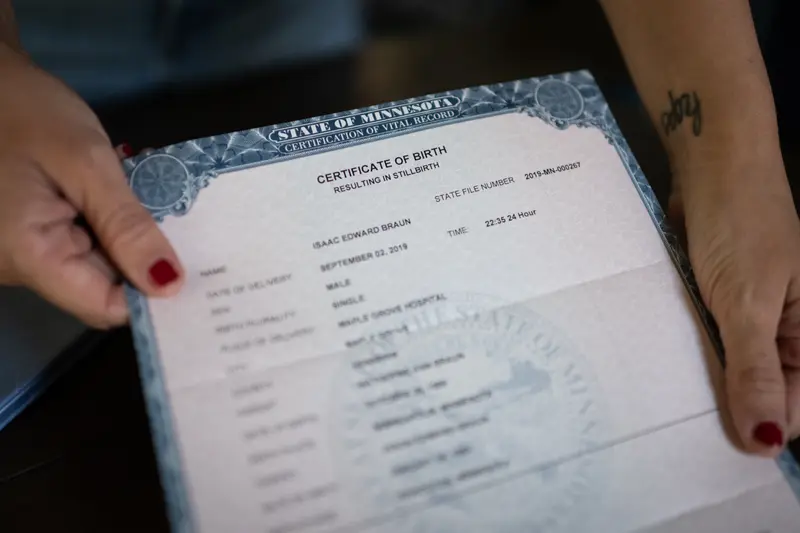
Less than two weeks before Jones’ stillbirth in Texas, Minnesota mother Kate Braun also delivered a stillborn boy at term. Braun and her husband, Jason, named him Isaac Edward, affectionately referring to him as Ike.
When the doctor told Braun, who was nearly 38 weeks pregnant, that her baby had died, she threw up. Then she sobbed uncontrollably before throwing up again.
Sue Steen, a nurse and stillbirth expert, walked Braun and her husband through the documents used to register the stillbirth with the state’s health department. They filled out two forms: one for the mother’s demographic information and another to capture the cause of death and medical information. Minnesota uses that information to create a fetal death record and, upon request from parents, a certificate of birth resulting in stillbirth.
“There’s something powerful about it being a formal document,” Braun said. “We have very few physical things to point to that validate his existence.”

Credit:
Caroline Yang, special to ProPublica
Not all causes of stillbirth can be determined. The CDC reported that in about 30% of stillbirths, the cause of death is unknown, and the way data is collected makes it difficult to know whether the cause couldn’t be medically determined or was just not recorded. A stunningly low number of autopsies exacerbates the problem, which is due in part to doctors not always offering the procedure to families and the federal government not covering its cost.
The CDC excludes states that have more than half of cases with unknown causes from its analysis. ProPublica found at least 10 states that did not meet that bar. In at least one year between 2019 and 2021, Georgia, Hawaii, Michigan, Mississippi, North Carolina, North Dakota, Vermont, Arizona, Wisconsin and New York were flagged for having insufficient data.
States registered the stillbirths but in many cases could not check off any of the dozens of causes that led to them because that information was not provided. State officials provided a variety of reasons for the lack of information. Although the hospital, doctor or parents in Arizona can submit the cause of death, “they often do not,” a spokesperson for the state Department of Health Services said. In hopes of improving its data quality, the state is working on hiring staff to reach out to the facilities that report data to the health department.
In Mississippi, which consistently has the worst stillbirth rate in the country, a state health department spokesperson said the agency doesn’t know if the information was not available or if the person completing the certificate didn’t retrieve it from the patient’s chart.
And while it’s possible to amend the fetal death certificate if the cause is later determined, it almost never happens, in part because the process often requires the person who signed the certificate to update it. Between 2019 and 2021 in Georgia, for instance, only 18 of nearly 2,000 stillbirths in the state that were missing a cause of death were updated.
Cause of death is only one of the many data points missing from stillbirth records. Year after year, states lacked data on crucial risk factors that could illuminate why a stillbirth happened, including cigarette smoking, diabetes, previous preterm births and blood pressure disorders.
In 2021, Washington state didn’t include any maternal risk factors in nearly 36% of stillbirths. Rhode Island was missing a similar percentage of information about cigarette use. And Washington, D.C., lacked information in more than 40% of its records about maternal prepregnancy weight, despite obesity being a risk factor for stillbirth.
In addition, important fetal data, such as information that could help indicate whether the fetus was growing as expected — another significant risk factor — was absent in many states. In 2021, New York — excluding New York City — Washington and Colorado were each missing birth weight in more than 20% of stillbirth records. That year, Hawaii was missing birth weight data in nearly 60% of cases.
More than 1,800 stillbirths nationally were missing race data in 2021, an increase from previous years. Race information is critical when considering the stark racial disparities in stillbirths overall and term stillbirths specifically. In an analysis for this story, ProPublica found that non-Hispanic Black women were about 1 1/2 times as likely as non-Hispanic white women to deliver a stillborn baby at or near their due date. Non-Hispanic Native Hawaiian or other Pacific Islander women were 2 1/2 times as likely to, compared with non-Hispanic white women.
Dr. Joy-Sarah Vink, a maternal fetal medicine specialist at Kapi‘olani Medical Center for Women & Children in Honolulu, wants to see stillbirth data reporting improve, especially when it comes to Native Hawaiian or other Pacific Islander women, who have among the highest rates of stillbirth in the U.S.
“There is no formal training for medical staff, no standardized training across the states as to how to best approach that,” she said.
As a Black woman, Jones had braced herself for the possibility of preeclampsia, a potentially fatal blood pressure condition that occurs during pregnancy that Black women are more likely to experience than white women. But she said no one told her about the risk of stillbirth, and especially not that it could happen days before her due date.

Credit:
Nitashia Johnson, special to ProPublica
Texas, like many states, requires a fetal death certificate to be completed within five days of the death and workers to ask parents for help with multiple fields, including mother’s race. But Jones said no one ever asked her for that information. Even in her pain, she said she wished they would have.
Jones went on to have two more boys, Kalan and Lawrence. But after years without a certificate for Giles that she could safely tuck away with her other sons’ birth certificates, she put in an expedited request in March to the Texas Department of State Health Services. In June, she received a certificate of birth resulting in stillbirth but has yet to get the fetal death certificate.
A Texas spokesperson said the agency cannot locate her request for the fetal death certificate but offered to expedite one. He said he understands the value of the document for grieving parents.
“It’s meaningful documentation,” Jones said. “It’s the legal proof of him existing.”
A certificate also would have saved her from uncomfortable conversations and the constant anguish of reliving her son’s death. Before Giles was born, she and her husband had reserved a spot for him at a day care center. After his stillbirth, Jones mustered the courage to call and tell them they wouldn’t need it anymore.
“Don’t go somewhere else,” the employee told her, thinking she had chosen another day care.
“No, no,” Jones sputtered.
Finally, she blurted out words no mother wants to say.
“He died.”